A cholesterol blood test, often called a lipid profile or lipid panel, measures different types of fat in your blood. It is one of the most common tests used to assess your risk of heart disease, stroke and problems caused by narrowed arteries.
Cholesterol results can be confusing because there is not just one number to look at. You may see total cholesterol, HDL cholesterol, non-HDL cholesterol, LDL cholesterol, triglycerides and a cholesterol ratio. Some numbers are better when they are lower. One, HDL cholesterol, is usually better when it is higher. Your age, sex, blood pressure, smoking status, diabetes history, kidney health, family history and previous heart problems also affect how your result should be interpreted.
This guide explains what each cholesterol result means, what may cause high or low results, when to speak to a GP or clinician, and what you can do next.
Important: This article is for general information only and should not replace medical advice. Cholesterol results should be interpreted in context, especially if you have diabetes, kidney disease, thyroid disease, liver problems, a history of heart disease or a strong family history of early heart attacks or strokes.
What is cholesterol?
Cholesterol is a fatty substance that your body needs in small amounts. It helps make cell membranes, hormones, vitamin D and bile acids, which help digest fats. Your liver makes cholesterol naturally, and you also get some from food.
The problem is not cholesterol itself. The problem is having too much of the wrong type of cholesterol circulating in the blood over time. Excess cholesterol can contribute to fatty deposits inside artery walls. This process is called atherosclerosis. It can slowly narrow the arteries and increase the risk of conditions such as angina, heart attack, stroke and peripheral arterial disease.
High cholesterol usually does not cause symptoms. Many people feel completely well until they have a blood test. That is why cholesterol testing is used as a risk assessment tool rather than a test you only have when you feel unwell.
What does a cholesterol blood test measure?
A full cholesterol blood test usually measures several related markers. Together, these give a better picture than total cholesterol alone.
Total cholesterol
Total cholesterol is the overall amount of cholesterol in your blood. It includes both “good” and “bad” types. It is useful as a broad marker, but it should not be interpreted on its own.
For example, two people could both have a total cholesterol of 5.5 mmol/L. One may have a high HDL cholesterol and a more reassuring profile. Another may have high LDL cholesterol, high triglycerides and a higher cardiovascular risk. The total number alone does not tell the whole story.
HDL cholesterol
HDL stands for high-density lipoprotein. It is often called “good cholesterol” because it helps remove cholesterol from the bloodstream and transport it back to the liver. A higher HDL cholesterol level is generally considered more favourable, although it is only one part of the overall risk picture.
Non-HDL cholesterol
Non-HDL cholesterol is calculated by subtracting HDL cholesterol from total cholesterol. It represents the cholesterol carried in all the potentially harmful particles, including LDL and other atherogenic lipoproteins.
In the UK, non-HDL cholesterol is commonly used because it gives a practical measure of “bad cholesterol” overall. The NHS explains that a cholesterol test may report total cholesterol, HDL cholesterol and non-HDL cholesterol, and that non-HDL is the difference between total cholesterol and HDL cholesterol. You can read more on the NHS cholesterol levels page.
LDL cholesterol
LDL stands for low-density lipoprotein. It is commonly called “bad cholesterol” because high levels can contribute to cholesterol build-up in artery walls. LDL cholesterol is often a key target when clinicians are deciding whether cholesterol-lowering treatment is needed.
LDL may be measured directly, but it is often calculated from other parts of the lipid profile. In some situations, such as very high triglycerides, the calculated LDL result may be less reliable.
Triglycerides
Triglycerides are another type of fat in the blood. They are not the same as cholesterol, but they are measured as part of a lipid profile because they also matter for cardiovascular and metabolic health.
Triglycerides can rise after eating, after alcohol intake, with weight gain, poorly controlled diabetes, some medicines, liver problems, kidney problems and inherited lipid disorders. Very high triglycerides can also increase the risk of pancreatitis, which is inflammation of the pancreas.
Total cholesterol to HDL ratio
The total cholesterol to HDL ratio compares your total cholesterol with your HDL cholesterol. A lower ratio is generally better. This ratio is sometimes used in cardiovascular risk calculators, but it should be interpreted alongside the rest of your lipid profile and your wider health history.
Cholesterol results: what is considered healthy in the UK?
Cholesterol results in the UK are usually measured in mmol/L. The following figures are commonly used as general guide values for adults, but your personal target may be different if you already have cardiovascular disease, diabetes, chronic kidney disease or a very high calculated risk.
| Cholesterol marker | General guide level | What it means |
|---|---|---|
| Total cholesterol | Below 5.0 mmol/L | Lower is generally better, but total cholesterol should not be interpreted alone. |
| Non-HDL cholesterol | Below 4.0 mmol/L | This reflects the main “bad cholesterol” burden overall. |
| LDL cholesterol | Below 3.0 mmol/L | Often a key treatment target, especially in people at higher cardiovascular risk. |
| HDL cholesterol | Above 1.0 mmol/L for men; above 1.2 mmol/L for women | Higher is usually more favourable, but very high HDL does not cancel out all other risks. |
| Triglycerides | Often below 1.7 mmol/L fasting, or below 2.3 mmol/L non-fasting | High levels may be linked with diet, alcohol, diabetes, weight, medicines or inherited causes. |
| Total cholesterol to HDL ratio | Usually lower is better; often below 6 is used as a broad guide | A risk-related ratio, but not the only number that matters. |
These guide levels are consistent with UK cholesterol information from organisations such as HEART UK, the British Heart Foundation and Lab Tests Online UK.
Why your cholesterol result is not just “normal” or “abnormal”
It is tempting to read cholesterol results as a simple pass or fail. In reality, cholesterol is about risk. A result that is mildly raised in one person may be less urgent than the same result in someone with diabetes, high blood pressure, chronic kidney disease or a previous heart attack.
For example, a 28-year-old non-smoker with normal blood pressure and no family history may be managed differently from a 62-year-old smoker with diabetes and high blood pressure, even if their cholesterol numbers look similar.
This is why doctors often combine cholesterol results with a cardiovascular risk assessment. In UK primary care, tools such as QRISK are commonly used to estimate the chance of developing cardiovascular disease over the next 10 years. NICE guidance on cardiovascular risk assessment and lipid modification recommends assessing overall cardiovascular risk rather than treating cholesterol numbers in isolation. You can read the NICE recommendations here: NICE NG238: cardiovascular disease risk assessment and reduction.
If you are trying to understand a full set of results, you may also find our general guide useful: How to Understand Blood Test Results.
What does high total cholesterol mean?
A high total cholesterol result means the overall amount of cholesterol in your blood is above the usual guide range. However, it does not show whether the increase is mainly due to HDL, LDL or other cholesterol-carrying particles.
If your total cholesterol is high, the next step is to look at your HDL, non-HDL, LDL and triglycerides. A high total cholesterol caused by high LDL or high non-HDL cholesterol is usually more concerning than a high total cholesterol caused mainly by a higher HDL cholesterol.
Common causes of high total cholesterol include a diet high in saturated fat, being physically inactive, carrying excess weight, smoking, drinking too much alcohol, type 2 diabetes, an underactive thyroid, kidney disease, liver or bile flow problems, some medicines and inherited conditions such as familial hypercholesterolaemia.
What does high LDL cholesterol mean?
High LDL cholesterol means there is more LDL cholesterol circulating in your blood than is ideal for your level of risk. LDL particles can enter artery walls and contribute to fatty plaque build-up over time.
High LDL cholesterol is especially important if you have other cardiovascular risk factors. These include:
- high blood pressure
- smoking
- diabetes
- chronic kidney disease
- a previous heart attack, stroke, angina or peripheral arterial disease
- a strong family history of early cardiovascular disease
- obesity or central weight gain
- South Asian, African or African-Caribbean background, where cardiovascular risk may be higher in some groups
LDL cholesterol can be affected by diet and lifestyle, but genetics are also important. Some people have high LDL cholesterol despite eating well and exercising regularly. This can happen in familial hypercholesterolaemia, an inherited condition that can cause very high cholesterol from a young age.
What does high non-HDL cholesterol mean?
High non-HDL cholesterol means the combined amount of cholesterol carried in the “bad” particles is raised. This includes LDL cholesterol and other particles that can contribute to artery disease.
Non-HDL cholesterol is useful because it does not require a fasting blood test and can give a broader picture of harmful cholesterol particles. Many UK cholesterol reports now include it.
If your non-HDL cholesterol is high, your clinician may consider your overall cardiovascular risk, lifestyle, blood pressure, blood sugar, kidney function, thyroid function and family history before advising on next steps.
What does low HDL cholesterol mean?
Low HDL cholesterol means your level of “good cholesterol” is lower than expected. Low HDL is associated with higher cardiovascular risk, especially when it appears alongside high triglycerides, insulin resistance, type 2 diabetes, smoking or excess abdominal weight.
Common reasons for low HDL cholesterol include smoking, physical inactivity, obesity, type 2 diabetes, high triglycerides, a diet high in refined carbohydrates, and some inherited factors.
Raising HDL itself is not usually the main treatment target. Instead, the focus is usually on improving the overall risk profile: lowering LDL or non-HDL cholesterol where needed, stopping smoking, increasing physical activity, improving diet, managing weight, controlling blood pressure and treating diabetes if present.
What does high HDL cholesterol mean?
Higher HDL cholesterol is generally considered favourable, but it does not make you immune from heart disease. A high HDL result does not cancel out very high LDL cholesterol, smoking, diabetes, high blood pressure or a strong family history.
If your HDL is high and your other results are healthy, that may be reassuring. But if your LDL, non-HDL cholesterol or triglycerides are high, you should still take the overall lipid profile seriously.
What do high triglycerides mean?
High triglycerides mean there is an increased level of this type of fat in your blood. Triglycerides often rise after food, so your result may be interpreted differently depending on whether the test was fasting or non-fasting.
Mildly raised triglycerides are common and may be linked to recent meals, alcohol, weight, insulin resistance or diabetes. Persistently high triglycerides may suggest metabolic syndrome, poorly controlled diabetes, excessive alcohol intake, liver problems, kidney problems, an underactive thyroid or an inherited lipid disorder.
Very high triglycerides need medical attention because they can increase the risk of pancreatitis. Pancreatitis can cause severe upper abdominal pain, nausea, vomiting and feeling very unwell. If you have severe abdominal pain, seek urgent medical help.
If your triglycerides are raised alongside abnormal liver enzymes, you may also find this article helpful: Liver Function Test Results Explained.
Do you need to fast before a cholesterol blood test?
Many cholesterol tests in the UK can now be done without fasting. NICE guidance states that before starting lipid modification therapy for primary prevention, at least one blood sample should be taken for a full lipid profile, including total cholesterol, HDL cholesterol, non-HDL cholesterol and triglycerides, and that a fasting sample is not needed.
However, there are times when a clinician may ask for a fasting sample. This may happen if your triglycerides are very high, if a previous result was difficult to interpret, or if a more detailed lipid assessment is needed.
If you are unsure whether to fast, follow the instructions from your GP surgery, clinic or testing provider. If you are having a private or home cholesterol test, check the sample instructions carefully before collecting your sample.
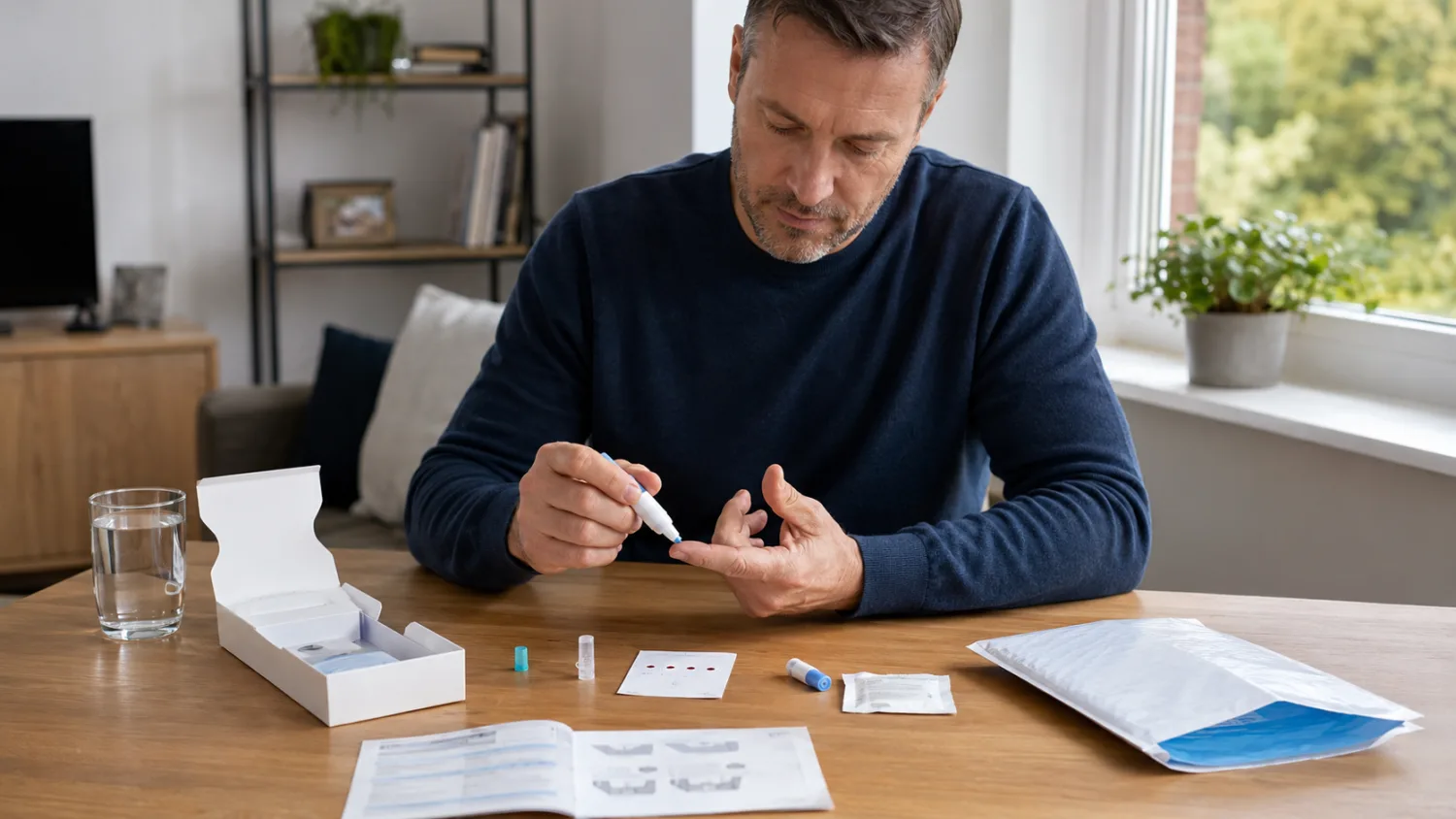
Finger-prick cholesterol tests vs venous blood tests
Cholesterol can be tested using a venous blood sample taken from a vein in the arm or, in some settings, a finger-prick sample. Both can be useful, but they are not always equivalent.
A venous blood sample sent to an accredited laboratory is generally the standard method for a full lipid profile. Finger-prick tests may be used for screening, home testing or quick checks, but the quality of the result can depend on the device, sample collection, timing, calibration, storage and laboratory process.
If you receive an unexpected, very high or concerning result from a home or finger-prick test, it is sensible to discuss it with a healthcare professional. They may recommend repeating the test using a venous sample, especially before making long-term treatment decisions.
What can affect cholesterol blood test results?
Cholesterol results can change for several reasons. A single result is useful, but it is only a snapshot.
Recent food and alcohol
Eating shortly before a test can particularly affect triglycerides. Alcohol can also raise triglycerides, especially if consumed heavily or in the days before the test.
Weight changes
Weight gain can worsen LDL cholesterol, non-HDL cholesterol and triglycerides. Weight loss, especially if achieved through a healthier diet and regular activity, can improve the overall lipid profile.
Illness or inflammation
Recent illness, infection or inflammation may affect blood results. If you have been acutely unwell, your clinician may recommend repeating the test later.
Thyroid disease
An underactive thyroid can raise cholesterol, particularly LDL cholesterol. If your cholesterol is unexpectedly high, your clinician may check thyroid function. You can read more here: Thyroid Blood Test Results Explained.
Diabetes and blood sugar control
Type 2 diabetes and insulin resistance can affect triglycerides and HDL cholesterol. Poor blood sugar control can worsen the lipid profile. If your cholesterol result is being assessed as part of diabetes risk, see: HbA1c and Blood Sugar Results Explained.
Kidney disease
Kidney disease can affect cholesterol and triglyceride levels and also increases cardiovascular risk. This means cholesterol targets and treatment decisions may be different. You can read more in our guide: Kidney Blood Test Results Explained.
Medicines
Some medicines can affect cholesterol or triglycerides. These may include steroids, some diuretics, some beta-blockers, some hormonal treatments, some immunosuppressants, some HIV medicines and certain acne treatments. Do not stop prescribed medicine without speaking to a clinician.
Pregnancy
Cholesterol and triglyceride levels naturally rise during pregnancy. Testing during pregnancy may be interpreted differently unless there is a specific clinical reason.
Genetics
Some people inherit a tendency to high cholesterol. Familial hypercholesterolaemia is one example. It can cause high LDL cholesterol from childhood or early adulthood and may increase the risk of early heart disease if untreated.
When could high cholesterol be inherited?
Inherited high cholesterol should be considered if your LDL cholesterol is very high, if high cholesterol was found at a young age, or if there is a family history of early heart attacks, strokes or sudden cardiac death.
Familial hypercholesterolaemia, often shortened to FH, is an inherited condition that affects how the body clears LDL cholesterol from the blood. People with FH can have high cholesterol even if they are slim, active and eat a healthy diet.
Possible clues include:
- very high LDL cholesterol
- heart disease in a close relative at a young age
- known familial hypercholesterolaemia in the family
- cholesterol deposits around the tendons or eyes
- high cholesterol that does not improve much with lifestyle changes alone
If this sounds relevant, speak to your GP. Family members may also need testing.
What happens after an abnormal cholesterol result?
What happens next depends on how abnormal the result is and what your overall cardiovascular risk looks like.
Your GP or clinician may:
- review your medical history and family history
- check your blood pressure
- calculate your cardiovascular risk using a tool such as QRISK
- check for diabetes using HbA1c or fasting glucose
- check thyroid, liver or kidney blood tests
- ask about smoking, alcohol, diet and exercise
- repeat the cholesterol test if the result is unexpected
- discuss lifestyle changes
- consider cholesterol-lowering medicine if your risk is high enough
Some people need medication even if they feel well. Others may be advised to make lifestyle changes first and repeat the test later. The decision is individual.
When is cholesterol-lowering medicine considered?
Cholesterol-lowering medicine may be considered if your risk of cardiovascular disease is high, if you have already had a heart attack, stroke, angina or peripheral arterial disease, or if you have certain conditions that increase risk, such as diabetes or chronic kidney disease.
Statins are the most commonly used cholesterol-lowering medicines. They reduce LDL cholesterol and help lower the risk of heart attacks and strokes in people who are at increased risk. Other medicines, such as ezetimibe, PCSK9 inhibitors, inclisiran or bempedoic acid, may be used in some circumstances depending on risk, cholesterol levels, response to treatment and tolerance.
Medication decisions should be made with a clinician. Your cholesterol number matters, but so does your overall risk, personal preferences, other medical conditions and the balance of benefits and possible side effects.
Can lifestyle changes improve cholesterol?
Yes. Lifestyle changes can improve cholesterol results and reduce cardiovascular risk. The biggest gains usually come from changes that are realistic enough to maintain long term.
Reduce saturated fat
Saturated fat can raise LDL cholesterol. Common sources include butter, ghee, lard, fatty meats, processed meats, cream, cheese, pastries, cakes and many takeaway foods. You do not have to remove every favourite food, but replacing saturated fats with healthier unsaturated fats can help.
Examples include using olive or rapeseed oil instead of butter, choosing nuts or seeds instead of biscuits, and eating oily fish, avocado or unsaturated spreads in place of high-saturated-fat options.
Eat more soluble fibre
Soluble fibre can help lower cholesterol. Good sources include oats, barley, beans, lentils, chickpeas, fruit, vegetables and psyllium husk.
A practical start is to have porridge or oat-based cereal, add beans or lentils to meals, and aim for a wide variety of plant foods each week.
Choose a heart-healthy eating pattern
A Mediterranean-style diet is often recommended for heart health. This means plenty of vegetables, fruit, beans, lentils, wholegrains, nuts, seeds, olive oil, fish and smaller amounts of red or processed meat, butter, cream and sugary foods.
Be physically active
Regular activity can improve triglycerides, HDL cholesterol, blood pressure, insulin sensitivity and weight. Brisk walking, cycling, swimming, dancing, gym sessions or sports can all help. The best exercise is the one you can repeat consistently.
Stop smoking
Smoking increases cardiovascular risk and can lower HDL cholesterol. Stopping smoking is one of the most powerful ways to reduce your risk of heart attack and stroke, even if your cholesterol is also being treated.
Limit alcohol
Alcohol can raise triglycerides and contribute to weight gain and high blood pressure. If your triglycerides are high, reducing alcohol can make a noticeable difference.
Manage weight if needed
If you are carrying excess weight, especially around the waist, modest weight loss can improve triglycerides, HDL cholesterol, blood pressure and blood sugar control. The aim should be sustainable change rather than crash dieting.
Can cholesterol be too low?
Low cholesterol is usually not a problem if it is the result of effective treatment in someone at high cardiovascular risk. In fact, people who have had a heart attack or stroke may be advised to aim for much lower LDL cholesterol than the general population.
However, unexpectedly low cholesterol without treatment may sometimes be linked with other health issues, such as malnutrition, overactive thyroid disease, liver disease, chronic illness or problems with absorption. It should be interpreted with the rest of your blood tests and symptoms.
If your cholesterol is unexpectedly low and you feel unwell, are losing weight unintentionally, or have abnormal liver or thyroid results, speak to a clinician.
Cholesterol and other blood tests
Cholesterol is often checked as part of a broader health screen. Other results can change how your cholesterol is interpreted.
For example, high cholesterol with a raised HbA1c may suggest increased cardiovascular risk linked with diabetes or prediabetes. High cholesterol with abnormal thyroid results may point towards an underactive thyroid. High triglycerides with abnormal liver function tests may be linked with fatty liver, alcohol intake or metabolic health. Abnormal kidney function may increase cardiovascular risk and influence treatment choices.
For a wider explanation of interpreting multiple results together, see How to Understand Medical Test Results.
Can you get a cholesterol test privately in the UK?
Yes. Cholesterol testing is available through GP surgeries, NHS Health Checks for eligible adults, pharmacies, private clinics and home testing providers. Private cholesterol tests may be sold as a single lipid profile or as part of a wider heart health, general health, diabetes, hormone or wellbeing panel.
If you choose a private cholesterol test, check what is included. A useful test should ideally provide more than total cholesterol alone. Look for total cholesterol, HDL cholesterol, non-HDL cholesterol, LDL cholesterol and triglycerides. Also check whether the sample is finger-prick or venous, whether the laboratory is appropriately accredited, and whether clinical support is available if the result is abnormal.
UKAS accreditation is one important quality marker for laboratories in the UK. UKAS explains that accreditation gives confidence that laboratories have the required competence, equipment and processes for testing. You can learn more from UKAS information for patients.
Should you use a home cholesterol test?
Home cholesterol tests can be useful for convenience, screening and monitoring, but they have limitations. A home test is only as good as the sample quality, instructions, laboratory process and interpretation that comes with it.
A home test may be reasonable if you want a general check and you understand what will happen if the result is abnormal. However, if you have symptoms, a history of heart disease, diabetes, kidney disease, very high cholesterol, or a strong family history of early heart disease, it is better to involve a GP or clinician.
If a home test result is very abnormal, surprising or inconsistent with previous results, do not panic — but do not ignore it either. Speak to a healthcare professional. A repeat venous blood test may be recommended.
When should you speak to a GP about cholesterol results?
You should speak to a GP, pharmacist or qualified clinician if:
- your total cholesterol, LDL cholesterol or non-HDL cholesterol is high
- your triglycerides are high, especially if very high
- you have diabetes, kidney disease, high blood pressure or thyroid disease
- you have had a heart attack, stroke, angina, TIA or peripheral arterial disease
- you have a strong family history of early heart disease or stroke
- you are under 40 and have very high cholesterol
- you have cholesterol deposits around the eyes or tendons
- you are unsure whether you need treatment
- you received an abnormal result from a private or home test
Seek urgent medical help if you have symptoms of a heart attack or stroke. Cholesterol itself usually does not cause symptoms, but cardiovascular events can be life-threatening.
Symptoms that need urgent help
Call 999 if you or someone else has symptoms that could suggest a heart attack or stroke.
Possible heart attack symptoms include chest pain or pressure, pain spreading to the arm, jaw, neck, back or stomach, shortness of breath, sweating, nausea, light-headedness or a feeling of impending doom.
Possible stroke symptoms include face drooping, arm weakness, speech problems, sudden confusion, sudden vision loss, severe dizziness, loss of balance or a sudden severe headache.
How often should cholesterol be checked?
How often you need cholesterol testing depends on your age, risk factors and previous results.
Adults in England aged 40 to 74 may be invited for an NHS Health Check, which includes cardiovascular risk assessment. People with diabetes, kidney disease, previous cardiovascular disease, familial hypercholesterolaemia or those taking cholesterol-lowering medicine may need more regular monitoring.
If you are on a statin or another lipid-lowering treatment, your clinician may repeat blood tests to check your cholesterol response and, in some cases, liver function. Do not stop treatment simply because your cholesterol improves; the improvement may be because the medicine is working.
How to read your cholesterol result step by step
If you have your result in front of you, try reading it in this order:
- Check the units. In the UK, cholesterol is usually reported in mmol/L.
- Look at total cholesterol. This gives a broad overview, but do not stop there.
- Check HDL cholesterol. This is the “good” cholesterol. Higher is generally better.
- Check non-HDL cholesterol. This is often one of the most useful “bad cholesterol” measures.
- Check LDL cholesterol. This is a key marker, especially if treatment is being considered.
- Check triglycerides. Consider whether the test was fasting or non-fasting.
- Consider your personal risk. Age, blood pressure, smoking, diabetes, kidney disease and family history matter.
- Look for related results. HbA1c, thyroid, liver and kidney blood tests can all affect interpretation.
- Ask what happens next. You may need lifestyle advice, repeat testing, a risk calculation or medication.
The bottom line
A cholesterol blood test is not just about one number. The most useful interpretation comes from looking at total cholesterol, HDL cholesterol, non-HDL cholesterol, LDL cholesterol, triglycerides and your overall cardiovascular risk.
High cholesterol is common and usually has no symptoms, but it is important because it can increase the risk of heart disease and stroke over time. The good news is that cholesterol risk can often be reduced through lifestyle changes, medication when needed, and proper management of related conditions such as high blood pressure, diabetes, thyroid disease and kidney disease.
If your result is abnormal, do not panic. Use it as a prompt to understand your risk and take the next sensible step. For many people, cholesterol testing is not bad news — it is an opportunity to prevent future problems.
Frequently asked questions
What is a good cholesterol result?
As a general UK guide, total cholesterol is often considered healthier below 5.0 mmol/L, non-HDL cholesterol below 4.0 mmol/L, LDL cholesterol below 3.0 mmol/L, HDL cholesterol above 1.0 mmol/L for men and above 1.2 mmol/L for women. However, your personal target may be lower if you have cardiovascular disease, diabetes, kidney disease or a high calculated risk.
Which cholesterol number is most important?
There is no single number that matters for everyone. LDL cholesterol and non-HDL cholesterol are often especially important because they reflect harmful cholesterol particles. However, clinicians also consider HDL cholesterol, triglycerides and your overall cardiovascular risk.
Is total cholesterol enough to assess heart risk?
No. Total cholesterol alone can be misleading because it includes both “good” and “bad” cholesterol. A full lipid profile gives a better picture.
What is non-HDL cholesterol?
Non-HDL cholesterol is your total cholesterol minus your HDL cholesterol. It represents the cholesterol carried in potentially harmful particles. It is commonly used in UK cholesterol interpretation.
What is LDL cholesterol?
LDL cholesterol is often called “bad cholesterol”. High LDL cholesterol can contribute to fatty build-up in artery walls and increase the risk of heart attack and stroke over time.
What is HDL cholesterol?
HDL cholesterol is often called “good cholesterol”. It helps remove cholesterol from the blood and transport it back to the liver. Higher HDL is generally more favourable, but it does not cancel out high LDL or other risk factors.
What are triglycerides?
Triglycerides are a type of fat in the blood. They can rise after food, alcohol, weight gain, diabetes, liver problems, kidney problems, some medicines and inherited conditions. Very high triglycerides can increase the risk of pancreatitis.
Do I need to fast before a cholesterol test?
Often, no. Many cholesterol tests can be done without fasting. However, fasting may be requested if your triglycerides are very high or if your clinician needs a more specific assessment.
Can stress raise cholesterol?
Long-term stress may indirectly affect cholesterol by influencing sleep, diet, alcohol intake, smoking, activity levels and weight. Stress alone is rarely the only reason for a high result, but it can contribute to an unhealthy risk pattern.
Can alcohol affect cholesterol results?
Yes. Alcohol can raise triglycerides and contribute to weight gain, high blood pressure and liver problems. If triglycerides are high, reducing alcohol is often recommended.
Can thyroid problems cause high cholesterol?
Yes. An underactive thyroid can raise cholesterol, especially LDL cholesterol. This is why thyroid function may be checked when cholesterol is unexpectedly high.
Can diabetes affect cholesterol?
Yes. Diabetes and insulin resistance can raise triglycerides, lower HDL cholesterol and increase cardiovascular risk. Cholesterol treatment thresholds may be different for people with diabetes.
Can high cholesterol cause symptoms?
Usually not. High cholesterol often causes no symptoms. It is normally found through a blood test. Rarely, inherited very high cholesterol can cause visible cholesterol deposits around the eyes or tendons.
Can I have high cholesterol if I am slim?
Yes. Slim people can still have high cholesterol due to genetics, diet, thyroid disease, kidney disease, liver problems, medicines or other factors. Body weight is only one part of the picture.
What cholesterol level needs medication?
There is no single cholesterol level where everyone automatically needs medication. The decision depends on LDL or non-HDL cholesterol, your overall cardiovascular risk, existing medical conditions, family history and whether you have already had cardiovascular disease.
Are statins always needed for high cholesterol?
No. Some people can improve cholesterol with lifestyle changes, especially if their overall risk is low. Others benefit from statins because their cardiovascular risk is higher. This should be discussed with a clinician.
How quickly can cholesterol improve?
Lifestyle changes can begin to improve cholesterol within weeks, but meaningful reassessment is often done after a few months. Medication can lower LDL cholesterol more quickly, but monitoring schedules vary.
Should I repeat an abnormal cholesterol test?
Sometimes. A repeat test may be useful if the result is unexpected, if triglycerides are very high, if the sample may have been affected by recent food or alcohol, or before making long-term treatment decisions.
Are home cholesterol tests accurate?
Some home cholesterol tests can be useful, but accuracy depends on sample collection, test quality, laboratory standards and interpretation. Unexpected or very abnormal home test results should be discussed with a healthcare professional and may need confirmation with a venous blood test.
What should I do if my cholesterol is high?
Do not panic. Look at the full lipid profile, consider your wider risk factors and speak to a GP, pharmacist or qualified clinician. You may need lifestyle changes, repeat testing, further blood tests, cardiovascular risk assessment or medication.