Spirometry is one of the commonest lung tests in the UK, and one of the easiest to misread once the numbers arrive. People often leave the appointment having heard terms like FEV1, FVC, “obstructive pattern”, “reversibility” or “normal for age”, without really knowing what any of it means. That can be frustrating, especially if the test was done because of ongoing cough, wheeze, breathlessness, chest tightness, smoking-related symptoms or suspected asthma or COPD. Spirometry measures how much air you can breathe out in one breath and how quickly you can blow it out, and it is used to check how well your lungs are working.
This guide is for UK patients who want a plain-English explanation of what spirometry can show, what the key numbers mean, why a result can be abnormal without being a crisis, and why a normal result does not always end the story. It is written to be useful whether you have already had the test or are waiting for results.
What spirometry actually measures
Spirometry is a breathing test done using a machine called a spirometer. You are usually asked to take the deepest breath you can, seal your lips around a mouthpiece, and then blow out as hard and fast as possible until your lungs feel empty. The machine records how much air you blow out and how quickly you do it. NHS guidance describes it as a lung function test used to look for problems with how well the lungs are working.
The results are not just one number. The spirometer produces several measurements, but in day-to-day practice the most important ones for patients to understand are FEV1, FVC and the FEV1/FVC ratio. Those three figures are what most of the clinical interpretation rests on.
Why people are sent for spirometry
Spirometry is commonly used when clinicians want to investigate symptoms such as long-term cough, wheeze, shortness of breath or reduced exercise tolerance. It is also used to help diagnose and monitor conditions including asthma, COPD and some other lung diseases. Asthma + Lung UK says spirometry can help explain symptoms like coughing or feeling short of breath and can be used to diagnose and monitor conditions such as asthma, COPD and pulmonary fibrosis.
A familiar example is the patient who has had an inhaler for months but has never had proper lung-function testing. Another is the ex-smoker with increasing breathlessness on hills. Another is the person whose cough keeps returning and whose doctor wants to know whether the airways are narrowed. The same test may be used in all of these cases, but the meaning of the result depends heavily on the symptoms, smoking history, age, medications and the timing of the test.
The three main spirometry numbers patients usually see
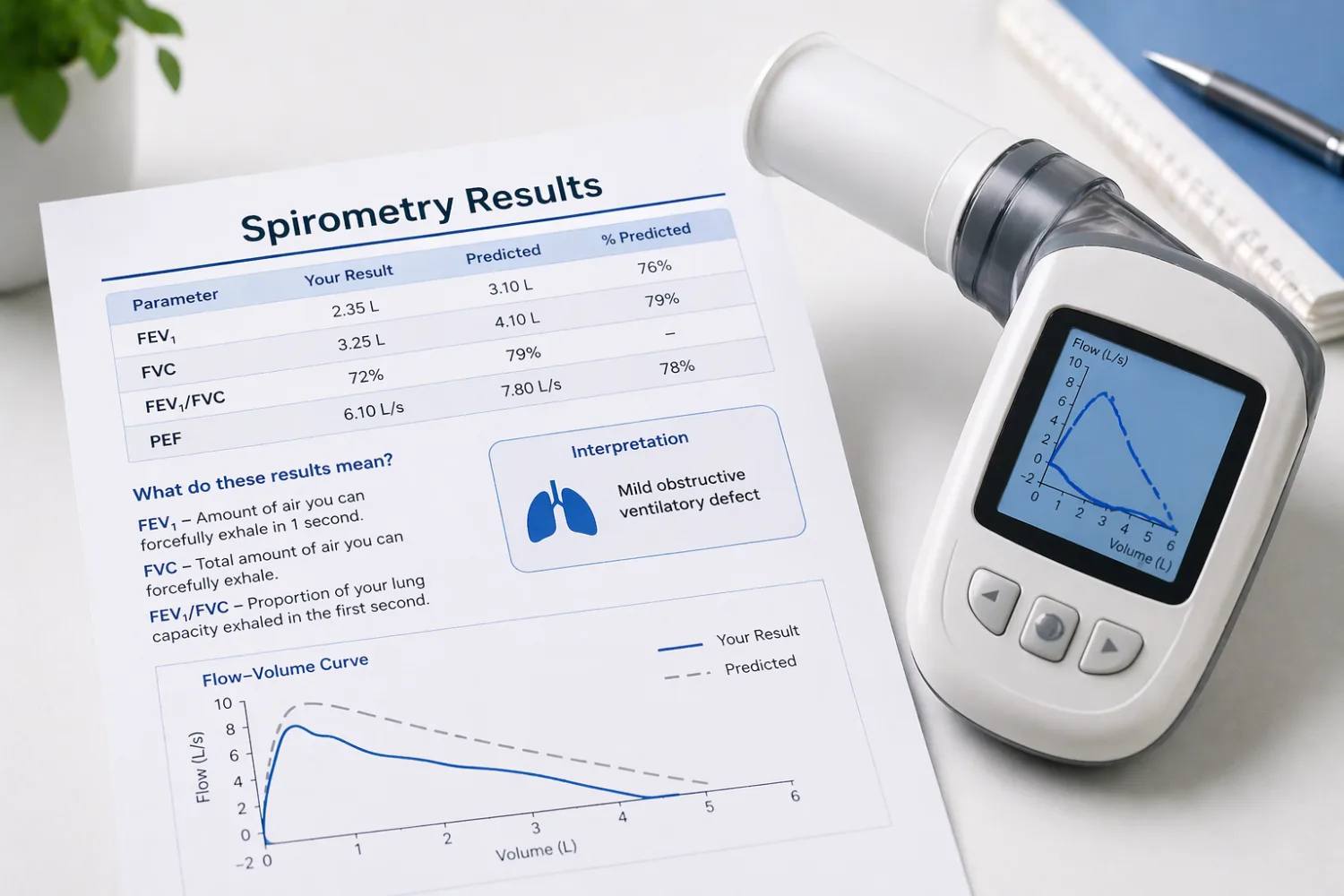
FEV1 stands for forced expiratory volume in one second. It tells you how much air you can blow out in the first second of a forced exhalation. FVC stands for forced vital capacity, which is the total amount of air you can blow out in one full forced breath. The FEV1/FVC ratio is the proportion of your total exhaled air that comes out in that first second. NHS-linked patient guidance and other UK lung-function leaflets use these same core definitions.
In healthy lungs, a large proportion of the air can usually be blown out in the first second, so the ratio stays relatively high. If the airways are narrowed or obstructed, less air comes out quickly, so the ratio drops. That is why the ratio is such a useful clue when doctors are looking for airflow obstruction.
What “predicted” and “percent predicted” mean
Spirometry reports often compare your measurements with “predicted” values. This simply means the machine compares your result with what would be expected for someone of your age, sex, height and sometimes ethnicity using reference equations. So if your report says FEV1 is 82% predicted, it means your result is 82% of what the machine would expect for a person with similar characteristics. UK spirometry guidance commonly reports FEV1, FVC and ratio alongside percent predicted values to help interpretation.
This is one reason patients should avoid comparing their raw numbers with a friend’s. The important question is not just the absolute number, but whether it is appropriate for you.
What an obstructive pattern means
An obstructive spirometry pattern usually means the airways are narrowed, inflamed or prone to collapse during forced exhalation, so air comes out more slowly than expected. In practice, this often shows up as a reduced FEV1/FVC ratio. In UK respiratory guidance, a post-bronchodilator FEV1/FVC ratio below 0.70 is commonly used to indicate persistent airflow obstruction in COPD.
This sort of pattern can be seen in conditions such as COPD and asthma, although the overall diagnosis depends on much more than the spirometry alone. For example, a smoker over 35 with chronic cough and breathlessness plus post-bronchodilator obstruction fits a very different picture from a younger person with variable wheeze whose results improve a lot after an inhaler. Asthma + Lung UK says spirometry is useful for diagnosing asthma and COPD, but the clinical context still matters.
What a restrictive pattern means
A restrictive pattern on spirometry usually means the total amount of air blown out is lower than expected, often because the lungs cannot expand fully or because of issues outside the lungs such as chest wall problems or weakness. On spirometry, this often appears as a reduced FVC with a ratio that is normal or high. But this is the critical bit: spirometry alone cannot definitively diagnose restrictive lung disease. Asthma + Lung UK’s ILD guidance specifically says that a reduced FVC may suggest a restrictive pattern, but restrictive lung disease cannot be diagnosed on spirometry alone.
That means a report saying “possible restrictive defect” is not the same as “you definitely have pulmonary fibrosis” or another serious scarring condition. It usually means the result may point in that direction and further tests, such as full lung volumes or imaging, may be needed.
What a normal spirometry result means
A normal result is reassuring, but it is not always the end of the story. If your FEV1, FVC and ratio are within the expected range, it means that at the time of the test your lung function did not show obvious airflow obstruction or a strong restrictive pattern. That is useful. But a normal spirometry result does not automatically rule out asthma, especially if you were well on the day of testing and your symptoms come and go. NHS England spirometry guidance and several UK clinical sources note that normal spirometry does not exclude asthma.
This is one of the commonest patient frustrations. Someone may have genuine episodes of wheeze, chest tightness and cough, yet have completely normal spirometry between flares. That does not mean the symptoms were imagined. It means the test caught you at a quieter moment.
Bronchodilator reversibility: why they sometimes repeat the test after an inhaler
Sometimes spirometry is done twice in one session: once before an inhaler and once again after you have taken a bronchodilator such as salbutamol. This is called bronchodilator reversibility testing. Its purpose is to see whether the airways open up after bronchodilator treatment. NHS patient information from hospital services explains that reversibility testing is done by performing spirometry before and after inhaled salbutamol to see whether narrowing of the airways is reversible.
This can be particularly helpful when asthma is being considered. Some UK asthma guidance uses an FEV1 increase of 12% and 200 mL or more after bronchodilator treatment as supporting evidence for asthma.
That said, reversibility is not a simple yes-or-no magic answer. A person with asthma may not show a dramatic response on the day, especially if they feel well or are already using inhalers. Equally, some improvement can happen in other airway diseases too. So the bronchodilator result helps, but it still has to be interpreted in context.
What spirometry can show in asthma
In asthma, spirometry may show airflow obstruction, especially during or near a symptomatic period. The FEV1/FVC ratio may be reduced, and the FEV1 may improve after bronchodilator treatment. But asthma is variable by nature, so results can sometimes be normal between episodes. UK asthma guidance repeatedly stresses that normal spirometry does not rule asthma out if the patient is well when tested.
A very ordinary example is the person who wheezes during pollen season, chest infections or exercise but attends the test on a good day. Their spirometry may be completely normal, and they may still need further objective testing or follow-up if the history is convincing. This article should therefore link naturally to your existing guides on hay fever and spring allergies in children, because airway symptoms often overlap in real life.
What spirometry can show in COPD
In COPD, spirometry is especially important because it is used to confirm persistent airflow obstruction rather than relying on symptoms alone. Asthma + Lung UK says spirometry is essential for diagnosing COPD, and that a post-bronchodilator FEV1/FVC ratio below 0.70 is commonly used to indicate persistent airflow obstruction.
Once airflow obstruction is confirmed, the FEV1 level can help describe severity, although doctors also look at symptoms, exacerbations, oxygen levels and the wider clinical picture. NHS England’s spirometry commissioning guidance notes that in the context of airflow obstruction, severity is reported using FEV1 and FEV1 percent predicted.
This matters because two patients may both have “COPD on spirometry” but be affected very differently in everyday life. One may be active with relatively mild symptoms. Another may be much more limited. The numbers matter, but they are not the whole condition.
Why you may need more than one blow, and why technique matters
Spirometry is not like stepping on a scale. The test depends on your effort and technique as well as the machine. You may need to repeat the blow several times so the operator can be confident the results are accurate and reproducible. NHS and hospital patient leaflets explain that the test is often repeated multiple times and that people may feel briefly light-headed from the forceful blowing.
This is important because a poor blow can make lungs look worse than they really are. Equally, someone who stops too early may have an FVC that looks falsely low, which can make a tracing appear “restrictive” when it is really just incomplete effort. That is one reason spirometry should be performed and interpreted by properly trained staff.
Why a result can be abnormal without meaning a serious illness
Like blood tests, spirometry results can be a clue rather than a diagnosis. A mildly reduced result may reflect temporary symptoms, suboptimal technique, smoking effects, recent infection, obesity, age-related changes or another factor that still needs interpretation. It may matter, but it is not always catastrophic. At the same time, you should not dismiss an abnormal result either. The right response is usually follow-up, not panic.
This is very similar to the way patients should think about other test reports: the number matters, but the pattern and context matter more. Your guide to how to understand blood test results is a strong internal companion piece for exactly that reason.
What happens if spirometry is abnormal
What happens next depends on the pattern. If there is clear airflow obstruction, doctors may think about asthma, COPD or other airway diseases and may look at smoking history, symptoms, reversibility and inhaler response. If there is a possible restrictive pattern, they may arrange fuller lung-function testing or imaging, because spirometry alone cannot confirm restriction. If the results are normal but symptoms continue, other tests such as peak flow monitoring, FeNO, chest imaging or repeat spirometry may be considered. Asthma + Lung UK and NHS-related guidance both present spirometry as one part of a broader respiratory work-up rather than the final word in every case.
This is also where other guides on your site can support readers. Someone with breathlessness may also benefit from reading ECG results explained, because shortness of breath is not always just a lung issue. Someone with smoking-related risk or cardiovascular concerns may also benefit from cardiovascular risk and high blood pressure.
Questions worth asking after spirometry
If you have been told your spirometry was normal or abnormal but you are not clear what that means, there are better questions than “Was it bad?” Ask whether the pattern was normal, obstructive or possibly restrictive. Ask whether the result fits asthma, COPD or something else. Ask whether bronchodilator reversibility was tested, whether the quality of the blows was good enough, and whether you need repeat spirometry or additional tests. Those questions usually lead to a much more useful conversation.
When breathlessness or wheeze should not wait for routine follow-up
Spirometry is usually a routine test, but the symptoms that led to it are not always routine. New or worsening breathlessness, chest pain, coughing up blood, blue lips, severe wheeze, or a sudden inability to speak in full sentences need urgent medical advice rather than waiting for a lung-function appointment. Spirometry helps assess chronic and diagnostic questions, but it is not a substitute for urgent assessment when symptoms are severe.
The bottom line
Spirometry is a very useful test that measures how much air you can blow out and how fast you can do it. The most important figures are FEV1, FVC and the FEV1/FVC ratio. A reduced ratio often points towards airflow obstruction, while a reduced FVC with a preserved ratio may suggest a restrictive pattern, although true restriction cannot be diagnosed on spirometry alone. A normal result is reassuring, but it does not always rule out asthma, especially if symptoms are intermittent.
The best way to think about spirometry is not as a final verdict but as a powerful piece of evidence. It tells clinicians a lot about how your lungs are behaving at the time of the test. The real meaning comes from combining that with your symptoms, history, smoking status, inhaler response and any further tests you may need.
Frequently asked questions
What is FEV1 on spirometry?
FEV1 is the amount of air you can forcefully blow out in the first second of a full exhalation. It is one of the main measurements used to assess lung function.
What is FVC?
FVC is the total amount of air you can blow out in one full forced breath after taking the deepest breath possible.
What does a low FEV1/FVC ratio mean?
A low FEV1/FVC ratio usually suggests airflow obstruction, meaning air is not coming out as quickly as expected. In COPD, a post-bronchodilator ratio below 0.70 is commonly used to indicate persistent airflow obstruction.
Can spirometry diagnose asthma?
It can support the diagnosis, especially if it shows variable airflow obstruction or improvement after a bronchodilator. But normal spirometry does not always rule asthma out, particularly if you are well on the day of testing.
Can spirometry diagnose COPD?
It is essential for confirming persistent airflow obstruction in suspected COPD, usually using a post-bronchodilator FEV1/FVC ratio below 0.70 in the right clinical context.
What does “possible restrictive pattern” mean?
It usually means the FVC is reduced in a way that may suggest restriction, but spirometry alone cannot confirm restrictive lung disease. Further tests are often needed.
Why do they repeat the test after an inhaler?
That is bronchodilator reversibility testing. It is done to see whether the airways open up after medication such as salbutamol, which can help when asthma is being considered.
Can spirometry be normal even if I have symptoms?
Yes. Symptoms such as asthma-related wheeze can be intermittent, so your spirometry may look normal between episodes.


